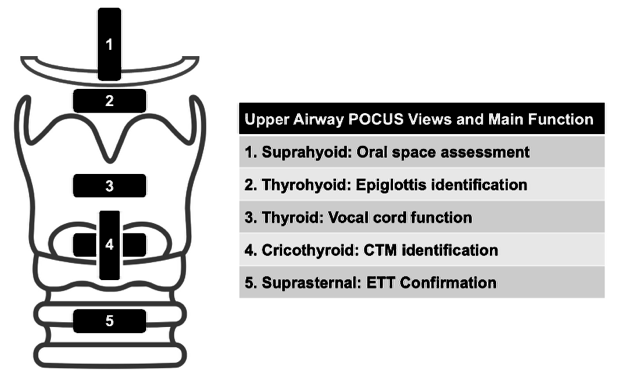
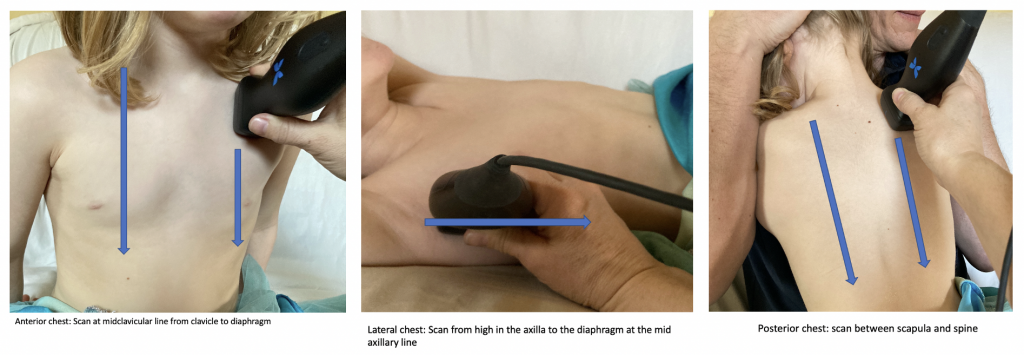
The airway can be evaluated by ultrasound from the suprahyoid area to the suprasternal notch in both the transverse and longitudinal planes (Figure 3). The transverse view is most commonly used to confirm the location of the ETT, but the longitudinal view can aid in landmarking when planning a surgical airway.
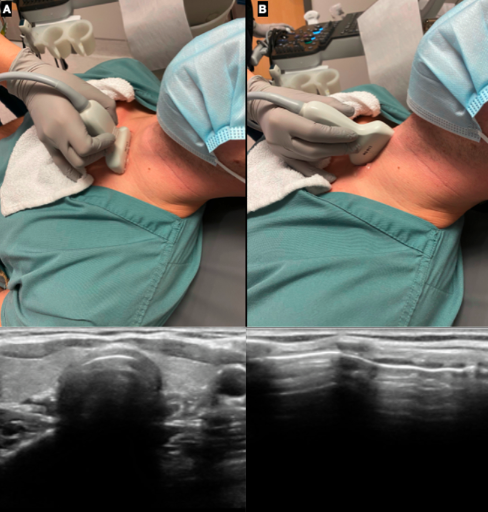
Figure 3. Airway POCUS using the linear probe in a supine patient in the A) transverse and B) longitudinal planes with corresponding sonographic appearance
Confirmation of ETT Position
Dynamic Technique
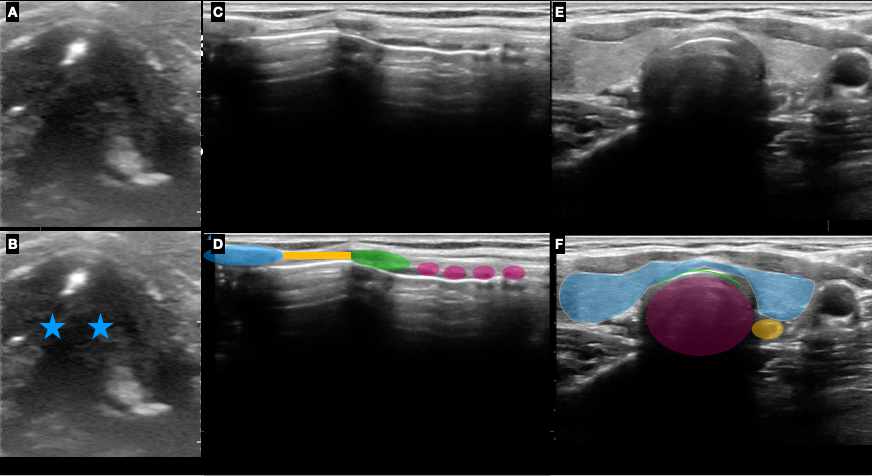
The dynamic evaluation is best performed with the probe in the transverse plane at the level of the suprasternal notch (Figure 3A). Identification of normal sonoanatomy including thyroid cartilage, air filled trachea and collapse esophagus (Figure 2 E-F) should be done before the intubation is started. In the majority of individuals, the esophagus will be left sided. However, it can also be positioned to the right or posterior to the trachea. Sonographers could adjust their scanning planes by slightly sliding and tilting the probe left and right to identify the position of the esophagus.
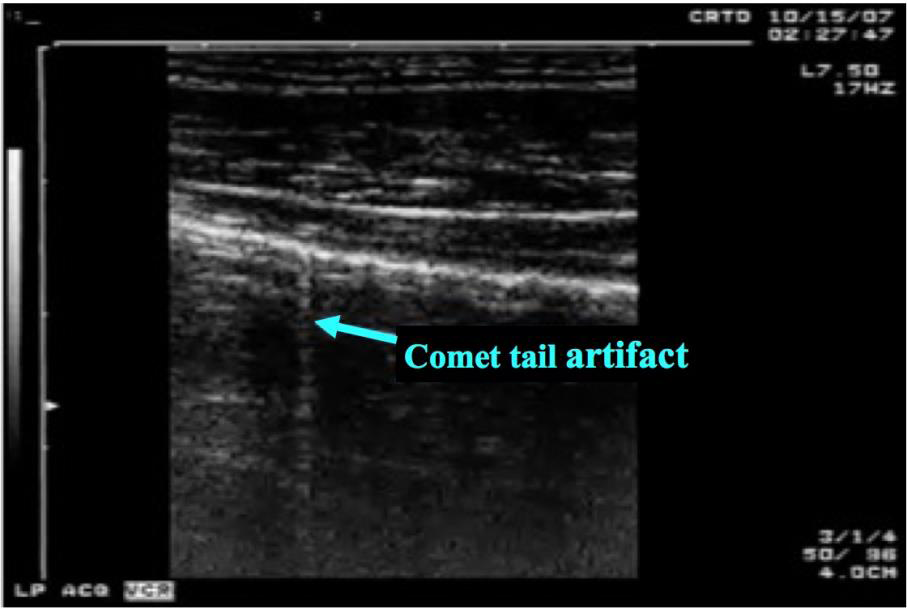
During endotracheal intubation, motion artefact (the snowstorm sign) will be visualized as the ETT is advanced in the trachea (Video 1). If the tube is inadvertently placed in the esophagus, a second air filled structure with comet tail artifact will appear, this is also called double trachea or double tract sign (Video 2).
Video 1: Transverse view of ETT advancement into the trachea with snowstorm sign.
Video 2: Transverse view of ETT placement within the esophagus (double trachea sign)
Advanced Technique
A more advanced technique is described in the literature: dynamic visualisation of ETT placement which can also be done at the level of the cricothyroid membrane in the transverse plane (Figure 1, level 3). In this position, the vocal cords are visualized and form an ‘A.’ This is called the triangle sign. When the ETT is passed in the trachea, brief movement is seen in this location, referred to as ‘snowstorm’ and then the vocal cords appear more spread out. This is called the bullet sign [16] (Figure 4 A-B).
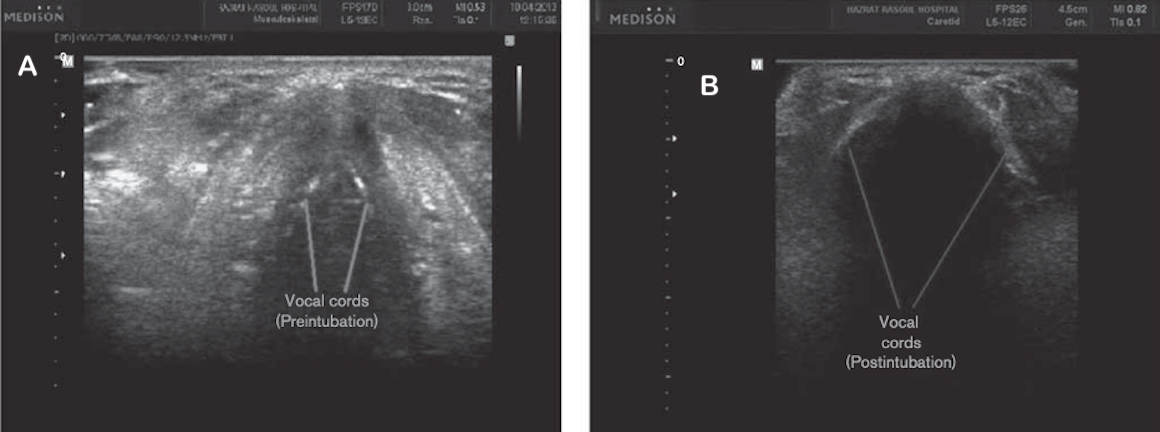
Figure 4: Dynamic movement of the vocal cords at the level of the cricothyroid membrane A) before intubation and B) after intubation
Static Technique
Static evaluation of tube placement is performed by placing the ultrasound probe in the suprasternal notch before the intubation to identify the sonoanatomy. Once the intubation is completed, the ultrasound is repeated. The image interpretation will be the same as the dynamic technique. With esophageal intubations, a second air filled structure with comet tail artifact will appear revealing the double tract sign (Figure 5).
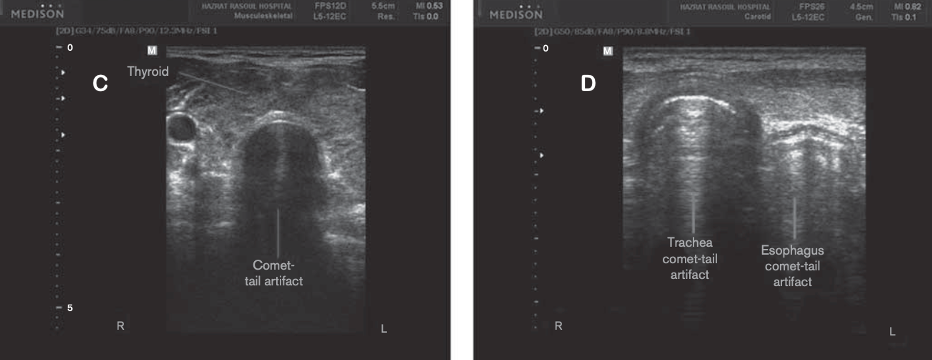
Figure 5: Transverse view with ultrasound position above the suprasternal notch showing comet tail artifact (c); and double-tract sign (d)