Indications
- Chest pain
- Dyspnea
- Blunt & penetrating trauma
- Unexplained hemodynamic instability
Equipment
- Ultrasound machine
- Phased Array (Cardiac) or Curvilinear (Abdominal) probe
- Ultrasound gel
Note: The small footprint and low frequency of the phased array probe make it ideal to generate images of the heart through the intercostal windows.
Technique
Pericardial effusions can be identified in all cardiac views, but we will focus on two with the highest yield: the subxiphoid view (also used in FAST scans) and the parasternal long axis view (PLAX). The other views (parasternal short view and apical four chamber view) have greater utility for other indications and will be reviewed in a separate module.
** For the purposes of this module, all views, probe orientation, and scanning instructions will follow the cardiology convention (screen indicator on the right). For guidance using the emergency medicine convention, please refer to the KidSONO Introduction to Cardiac Windows module**
Getting Started:
-
- Place the ultrasound machine so it is easily viewed while scanning.
- Ensure the patient is in the supine position.
- Drape the patient to allow access to both the abdomen and anterior chest.
- Set the ultrasound machine to an abdominal or cardiac setting, with the screen indicator on the left.
- If assessing for pericardial effusion as part of a FAST/EFAST examination, the abdominal preset may sometimes be selected, in which case the screen indicator may appear on the left in the emergency medicine convention
- You may use either the curvilinear or phased array probe.
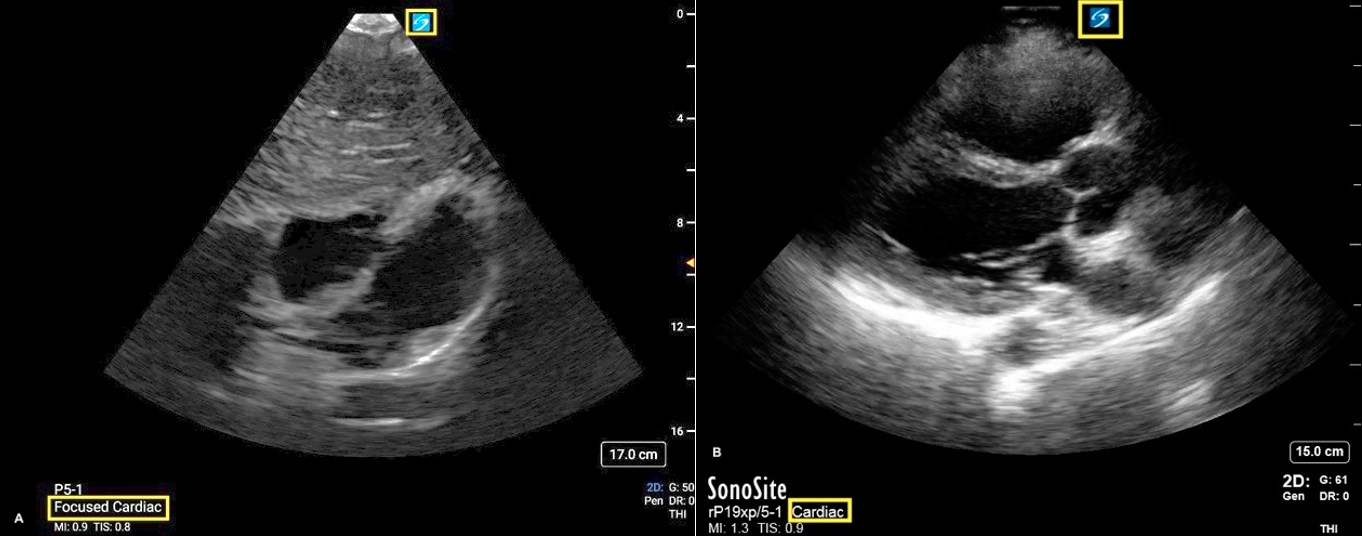
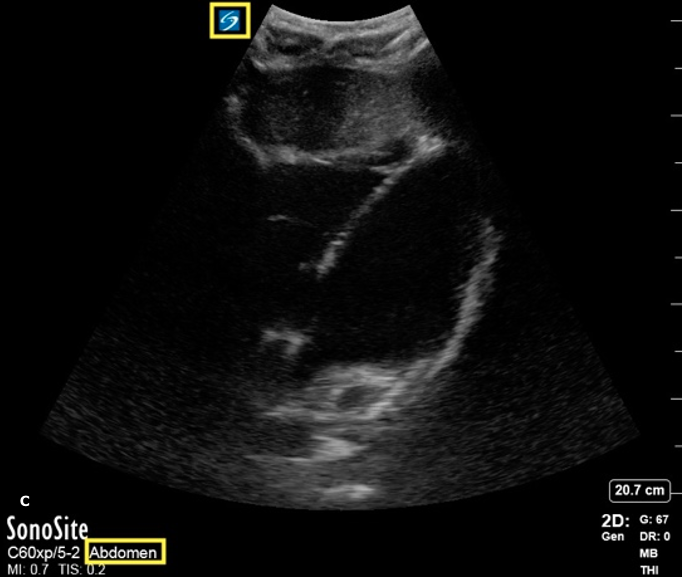
Figure 1: Subxiphoid (A) and PLAX (B) views with the phased array probe/cardiac preset and screen indicator position highlighted. (C) Subxiphoid view with the curvilinear probe/abdominal preset with screen indicator highlighted
Subxiphoid View
1. Place the probe inferior to the xiphoid process.
2. Ensure the probe marker is directed towards the patient’s left.
3. The probe will typically be angled about 15 degrees upward from the surface of the abdomen.
· Place your hand on top of the probe to facilitate the shallow angle of this view.
4. Aim the probe towards the patient’s left shoulder.
5. Use the liver as your acoustic window (the liver will be seen in the near field).
6. Identify the heart, including the posterior border of the heart, RV, septum and LV.
· These structures should make the shape of a ‘7’ on the screen.
7. Sweep SLOWLY through the heart from anterior to posterior.
· Identify any anechoic fluid collection in the pericardium.

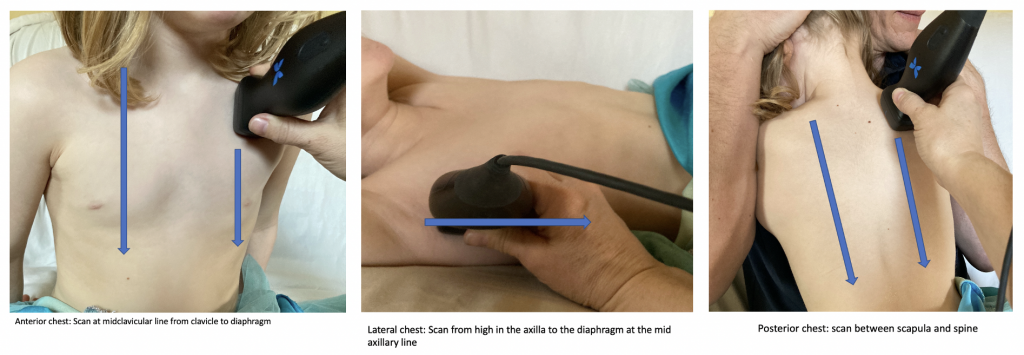
FIGURE 2: Probe position subxiphoid view
Troubleshooting Steps
- Ask patient to bend their knees to release tension on abdominal wall.
- Continue to advance the probe superiorly until you reach the xyphoid process.
- Use generous amounts of gel to minimize needing to “dig” under the xyphoid process.
- Ask the patient to “take a deep breath and hold it” to bring the heart closer to the probe.
- The image will improve as the probe moves closer to the heart.
Parasternal Long View
1. Identify the 3-4th intercostal space along the left sternal border.
2. Direct the probe marker towards the patient’s right shoulder.
3. Ensure the probe is directly perpendicular to the patient’s chest wall.
4. Identify the following:
· Near field: right ventricle
· Middle field: left ventricular outflow tract, left atrium, mitral valve, left ventricle
· Far field: descending aorta
5. Assess for an anechoic fluid collection in the pericardium, deep to the myocardium of the LA and LV.
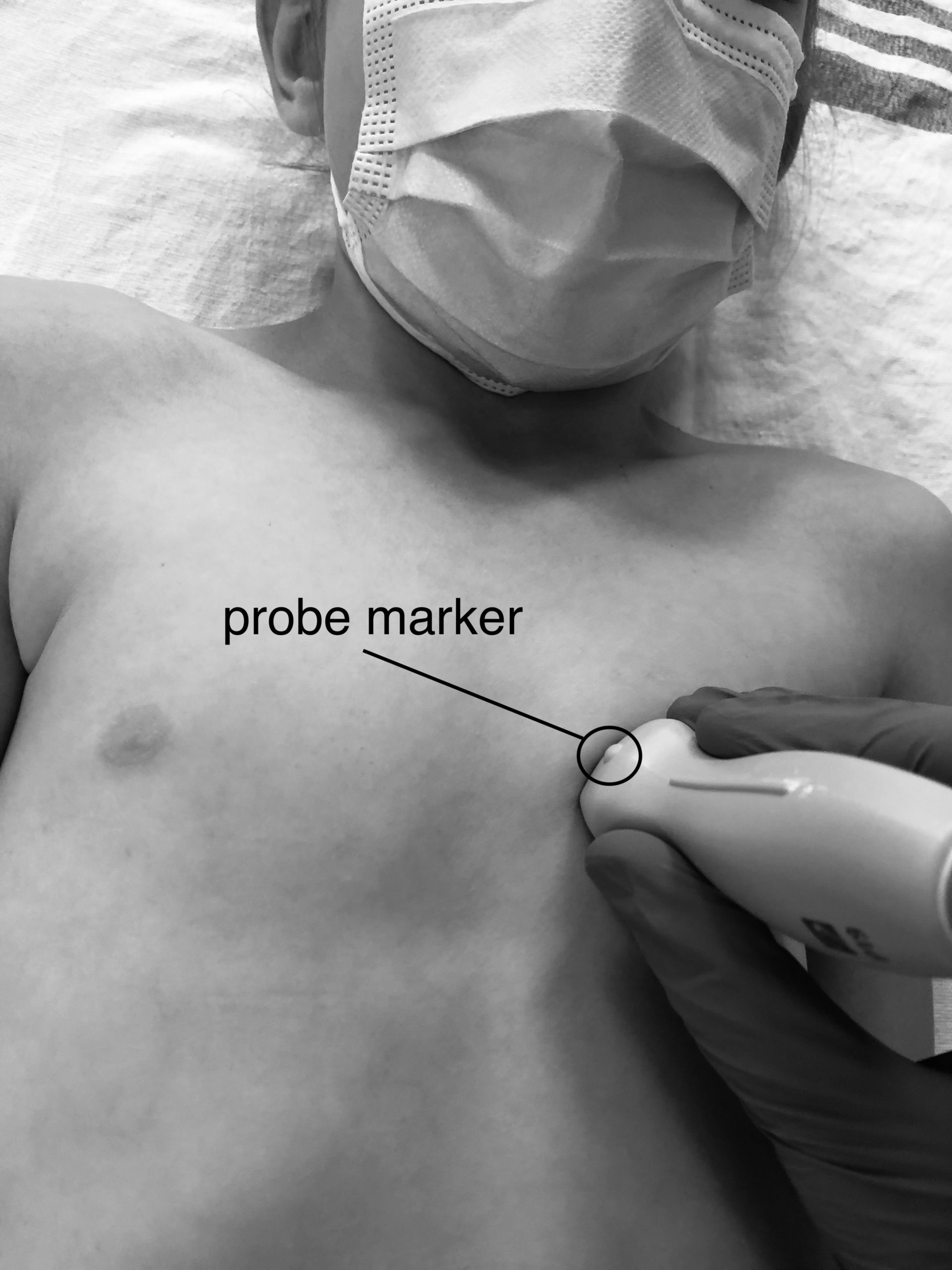
FIGURE 3: Probe position parasternal long view
Troubleshooting Steps: Lung Shadow
- Ask the patient to breathe out completely and hold – helps to remove the lung shadow.
- Rolling the patient into the left lateral decubitus position can also bring the heart closer to the chest wall and decrease the lung shadow.