A wide range of etiologies can lead to reduced left ventricular function (LVfx) in children, including cardiomyopathies, myocarditis, congenital heart defects (CHDs), sepsis, tachyarrhythmias, and chemotherapy-related toxicity, among others. These wide-ranging and clinically significant conditions highlight the importance of assessing cardiac function in pediatric patients.
Physical exam findings of cardiac dysfunction are often subtle or non-specific. The standard of care typically involves physical exam combined with the ordering of indirect tests such as EKG, CXR and troponins in the case of suspected LV dysfunction. A formal cardiology echocardiogram, interpreted by a cardiologist, is recommended if the index of suspicion is high. The reliance on formal echo is expensive and can delay diagnosis and compromise patient care, particularly during overnight or weekend hours when cardiology services may be limited.
Point-of-care ultrasound (PoCUS) has emerged as an important tool in the assessment of cardiac function, offering more timely and focused clinical insights than physical exam alone. Additionally, PoCUS findings can provide cardiologists with relevant preliminary information that helps streamline decision-making and enhance patient care.
This module focuses on guiding learners through a preliminary assessment of LVfx using PoCUS. While the evaluation of CHDs and valvular abnormalities is common in pediatric cardiology, these are beyond the scope of of this module. By course completion, learners should feel confident assessing global LVFx using the five standard PoCUS cardiac views.
Why Ultrasound?
Ultrasound’s advantages include being low cost, portable, and free from ionizing radiation. This, in addition to its ability to visualize the heart and its function in real time, makes it the diagnostic modality of choice for cardiac evaluation [1]. PoCUS is now widely available in most emergency departments (EDs), intensive care units (PICUs) and hospital wards, providing rapid, real-time evaluation of cardiac function in critically ill patients.
When managing patients with respiratory or circulatory compromise, prompt and accurate diagnosis is crucial. Adult studies have demonstrated that PoCUS enables clinicians to diagnose more quickly and accurately than clinical assessment alone, facilitating more targeted and timely interventions [2,3] and in some cases, improving mortality outcomes [4,5].
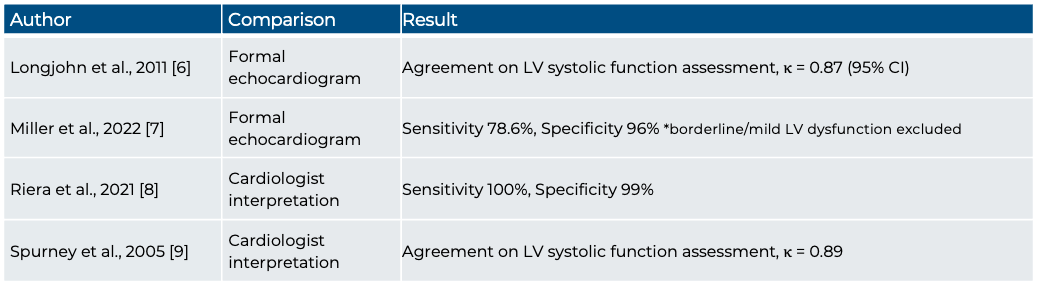
Several studies have shown that pediatric physicians without cardiology specialization can reliably assess left ventricular (LV) systolic function using cardiac PoCUS following appropriate training [6-10], including hypotensive patients [11]. Reported diagnostic performance has been high, with studies demonstrating excellent agreement with formal echocardiography (κ = 0.87–0.89) [6,9].
Table 1: Diagnostic Accuracy of POCUS for LVfx assessment in pediatric populations
Cardiac function PoCUS generally utilizes an impression-based, qualitative approach, whereas formal echocardiography relies more on quantitative measures. That said, PoCUS is supported by one or two key semi-quantitative measures, such as the E-Point Septal Separation (EPSS), which has demonstrated high negative predictive value in ruling out systolic dysfunction in pediatric patients [12], highlighting its utility as a screening tool.
PoCUS is also repeatable, allowing practitioners to monitor the effectiveness of interventions and changes in LVfx over time. PoCUS is a skill that can be learned and acquired through training, including both didactic and hands-on practice. Research supports that once undergoing short training, PoCUS can safely and accurately be used by practitioners at the bedside in both adult and pediatric populations [2, 13-17]. Given these benefits, PoCUS use for cardiac assessments is now endorsed by multiple professional societies [18,19].

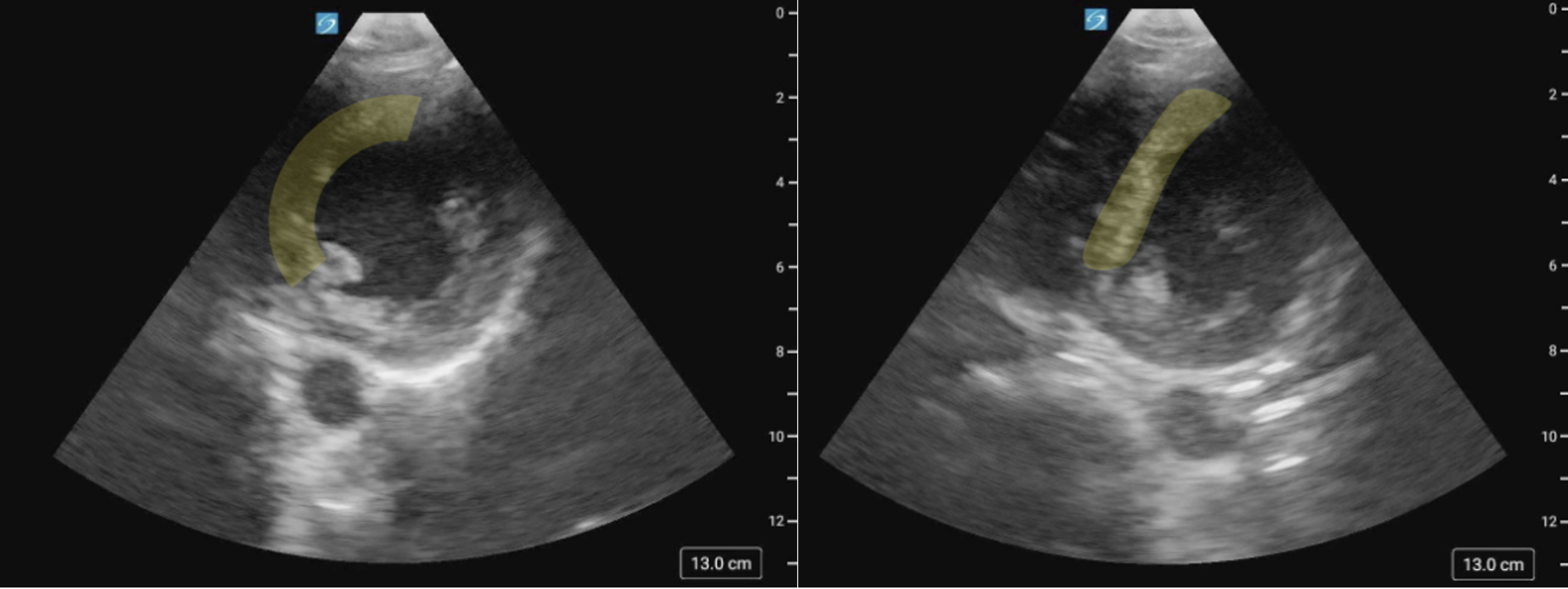
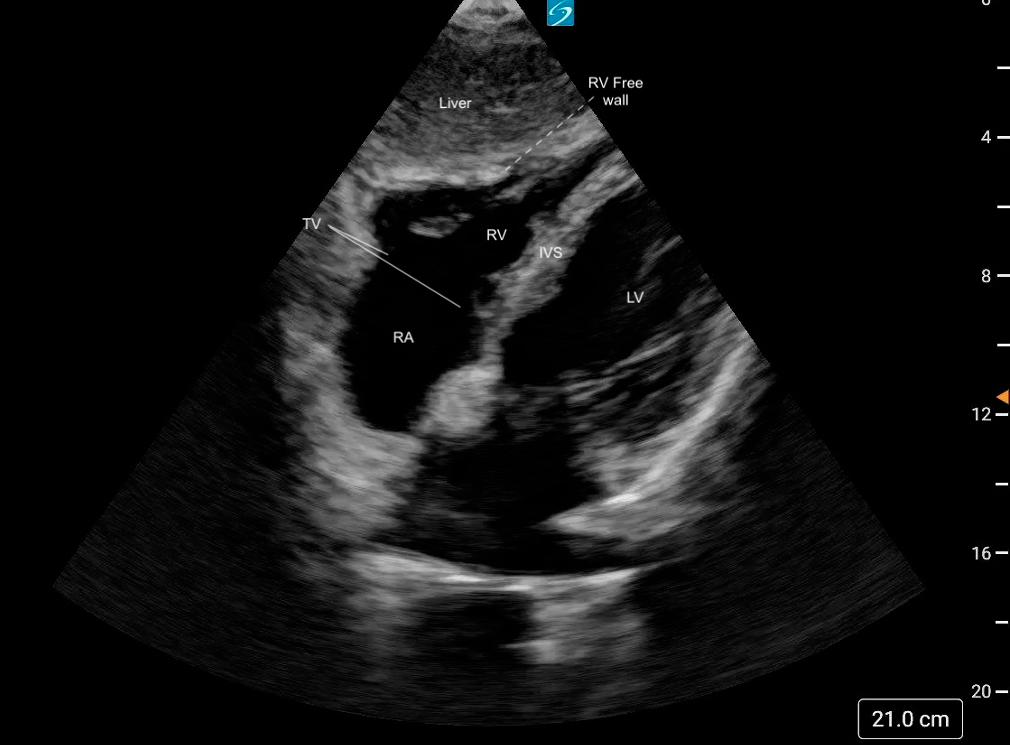

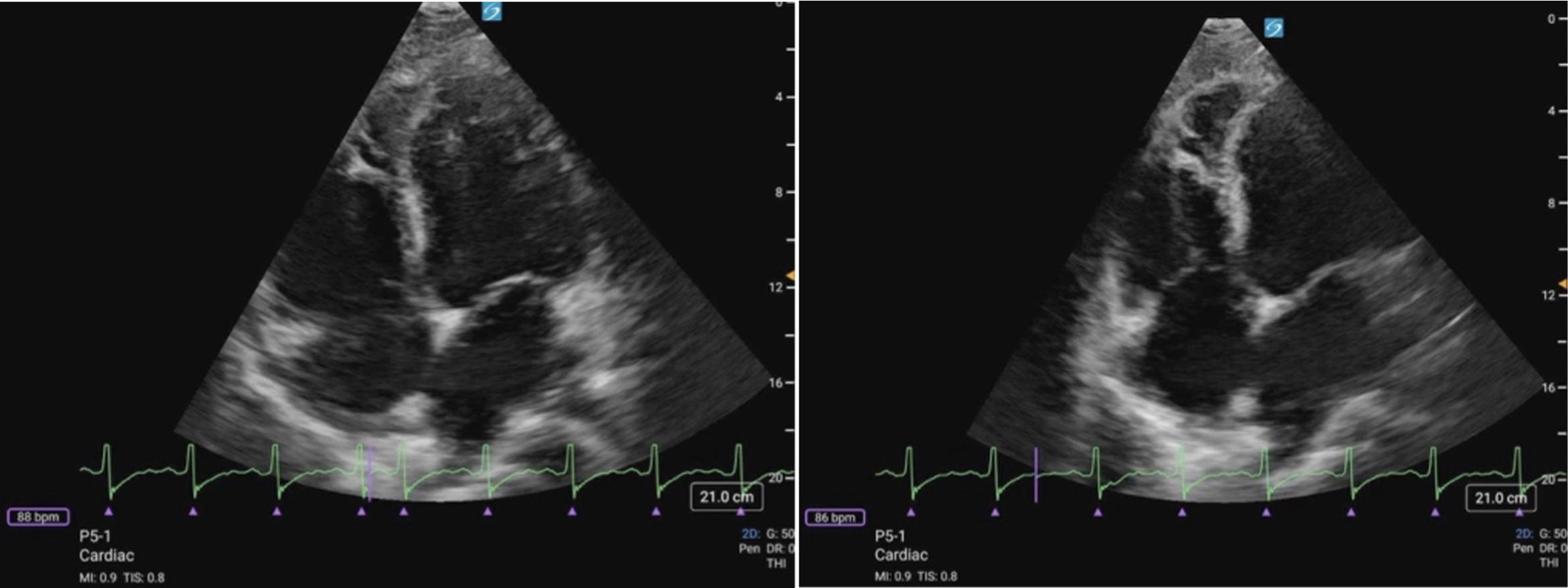 Figure 11 (a) A4C Cardiology convention LV focused compared to (b) RV focused. Note how in the RV focused view, the LV may be out of frame, but the RV free wall and apex are fully visualized.
Figure 11 (a) A4C Cardiology convention LV focused compared to (b) RV focused. Note how in the RV focused view, the LV may be out of frame, but the RV free wall and apex are fully visualized.