Pitfalls
As with all PoCUS imaging, care must be taken to understand the limitations of imaging the kidney and collecting duct system. First, care must be taken to avoid incorrectly ascribing hydronephrosis due to obstruction in a patient with a full bladder or one who is over hydrated. Ideally patients undergoing evaluation of the urinary tract should be well hydrated, but not overly so, and have a partly filled, but not distended bladder. Care must also be taken not to mistake prominent hypoechoic renal pyramids in pediatric patients for hydronephrosis. Their location is outside the renal sinus in contrast to hydronephrosis, which always occurs inside the renal sinus.
In addition, PoCUS imaging is limited for direct visualization of suspected renal calculi. Nephrolithiasis is possible even if the stone cannot be visualized. Lastly, the absence of hydronephrosis does not rule out a renal stone as small stones may not cause hydronephrosis. If hydronephrosis is detected on PoCUS, further evaluation with a formal ultrasound by radiology, and potentially a KUB X-ray, is recommended to assess for the presence and size of renal stones.
Lastly, there are several normal or pathological findings that can be misinterpreted as hydronephrosis on ultrasound. Careful technique and interpretation are essential to avoid false positives. These include:
- Extrarenal Pelvis: a normal and often benign anatomical variant that lies predominantly outside the renal sinus. An extrarenal pelvis on ultrasound will appear as an anechoic structure adjacent to the renal sinus without any pelviectesis, caliectasis, or cortical thinning. You can also place color doppler over it to make sure there is no arterial or venous flow present. (Figure 18)
- Parapelvic Cysts: non-malignant, fluid-filled anechoic structures formed near the renal pelvis and therefore can be mistaken for hydronephrosis. The anechoic areas of cysts are localized and do not connect to the calyces. They are round or oval making them distinguishable from hydronephrosis. Any findings of suspected renal cysts should be followed up with a formal renal ultrasound. (Figure 19)
- Prominent renal arteries/veins and Renal Vascular Malformations can also cause false positives for hydronephrosis. Color Doppler indicates blood flow and can distinguish renal prominent vessels or vascular malformations from hydronephrosis.(Figure 20)
- Polycystic Kidney Disease (PCKD) and Acquired Renal Cystic Disease (ARCD) are diseases in which there will be an abundance of irregular renal cysts of varying size that distort the kidney’s shape bilaterally and can sometimes be mistaken for severe hydronephrosis. (Figure 21)
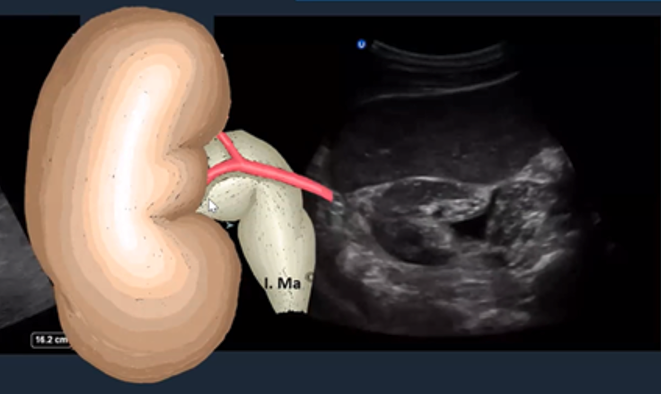 Figure 18: Short axis of the right kidney with an extra renal pelvis. [12]
Figure 18: Short axis of the right kidney with an extra renal pelvis. [12]
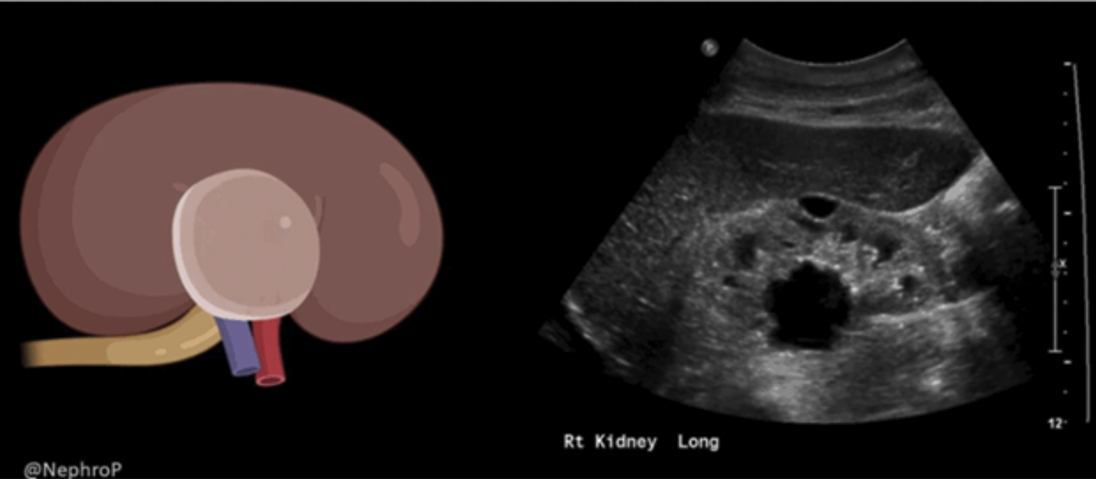 Figure 19: Sagittal image of the right kidney with a parapelvic cyst. Image use with permission from Nephro POCUS [15]
Figure 19: Sagittal image of the right kidney with a parapelvic cyst. Image use with permission from Nephro POCUS [15]
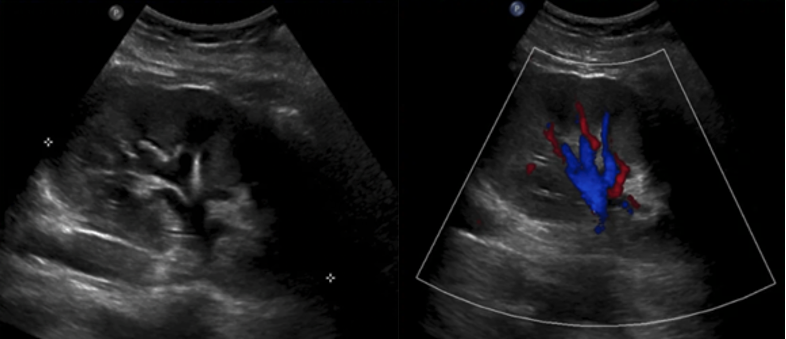 Figure 20: Sagittal 2D and color image of the kidney with prominent vasculature at the renal pelvis. Image use with permission from Nephro POCUS [15]
Figure 20: Sagittal 2D and color image of the kidney with prominent vasculature at the renal pelvis. Image use with permission from Nephro POCUS [15]
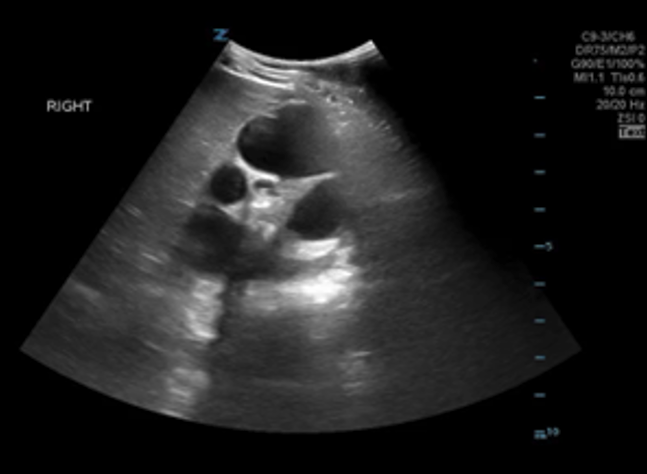 Figure 21: Sagittal image of a kidney with PCKD
Figure 21: Sagittal image of a kidney with PCKD

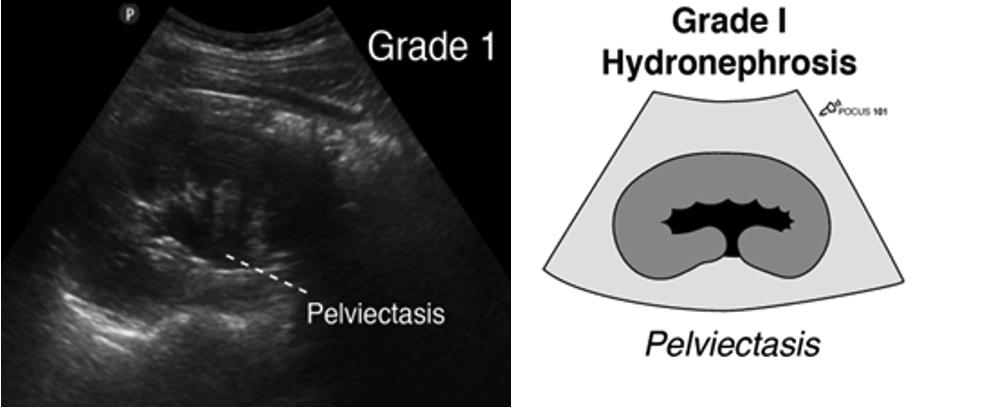 Figure 11: Longitudinal ultrasound image of the kidney with corresponding anatomical diagram, demonstrating pelviectasis. Image use with permission POCUS 101 [10].
Figure 11: Longitudinal ultrasound image of the kidney with corresponding anatomical diagram, demonstrating pelviectasis. Image use with permission POCUS 101 [10].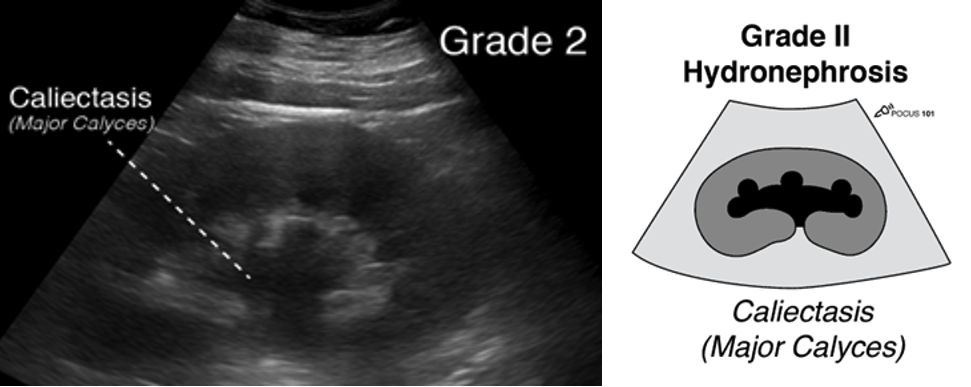 Figure 12: Longitudinal ultrasound image of the kidney with matching anatomical illustration, showing pelviectasis and dilation of the major calyces. Image use with permission POCUS 101 [10].
Figure 12: Longitudinal ultrasound image of the kidney with matching anatomical illustration, showing pelviectasis and dilation of the major calyces. Image use with permission POCUS 101 [10].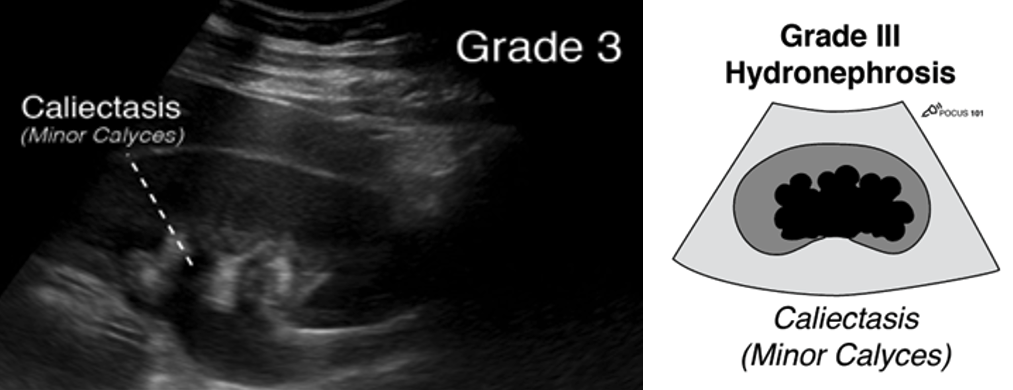 Figure 13: Longitudinal ultrasound image of the kidney with matching anatomical illustration, showing pelviectasis and dilation of the major and minor calyces. Image use with permission POCUS 101 [10].
Figure 13: Longitudinal ultrasound image of the kidney with matching anatomical illustration, showing pelviectasis and dilation of the major and minor calyces. Image use with permission POCUS 101 [10].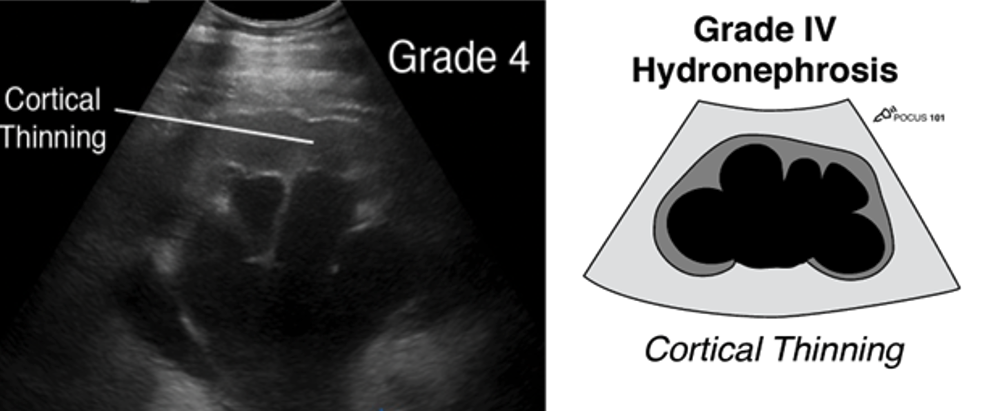 Figure 14: Longitudinal ultrasound image of the kidney with matching anatomical illustration, showing pelviectasis, caliectasis and cortical thinning. Image use with permission POCUS 101 [10]
Figure 14: Longitudinal ultrasound image of the kidney with matching anatomical illustration, showing pelviectasis, caliectasis and cortical thinning. Image use with permission POCUS 101 [10]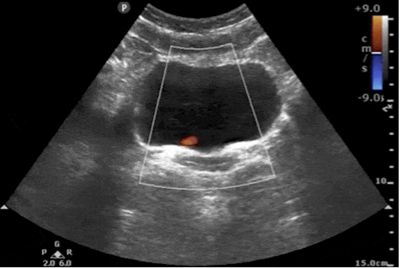 Figure 15: Transverse bladder with absent left uretic jet
Figure 15: Transverse bladder with absent left uretic jet Figure 16: Sagittal image of the right kidney with a large stone displaying posterior enhancement in the lower pole. Image use with permission POCUS 101 [10].
Figure 16: Sagittal image of the right kidney with a large stone displaying posterior enhancement in the lower pole. Image use with permission POCUS 101 [10].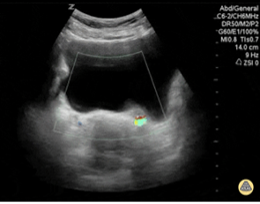 Figure 17: Transverse color image of the bladder showing twinkle artefact at the left UVJ indicative of a stone. Image use with permission from POCUS Atlas [12]
Figure 17: Transverse color image of the bladder showing twinkle artefact at the left UVJ indicative of a stone. Image use with permission from POCUS Atlas [12]


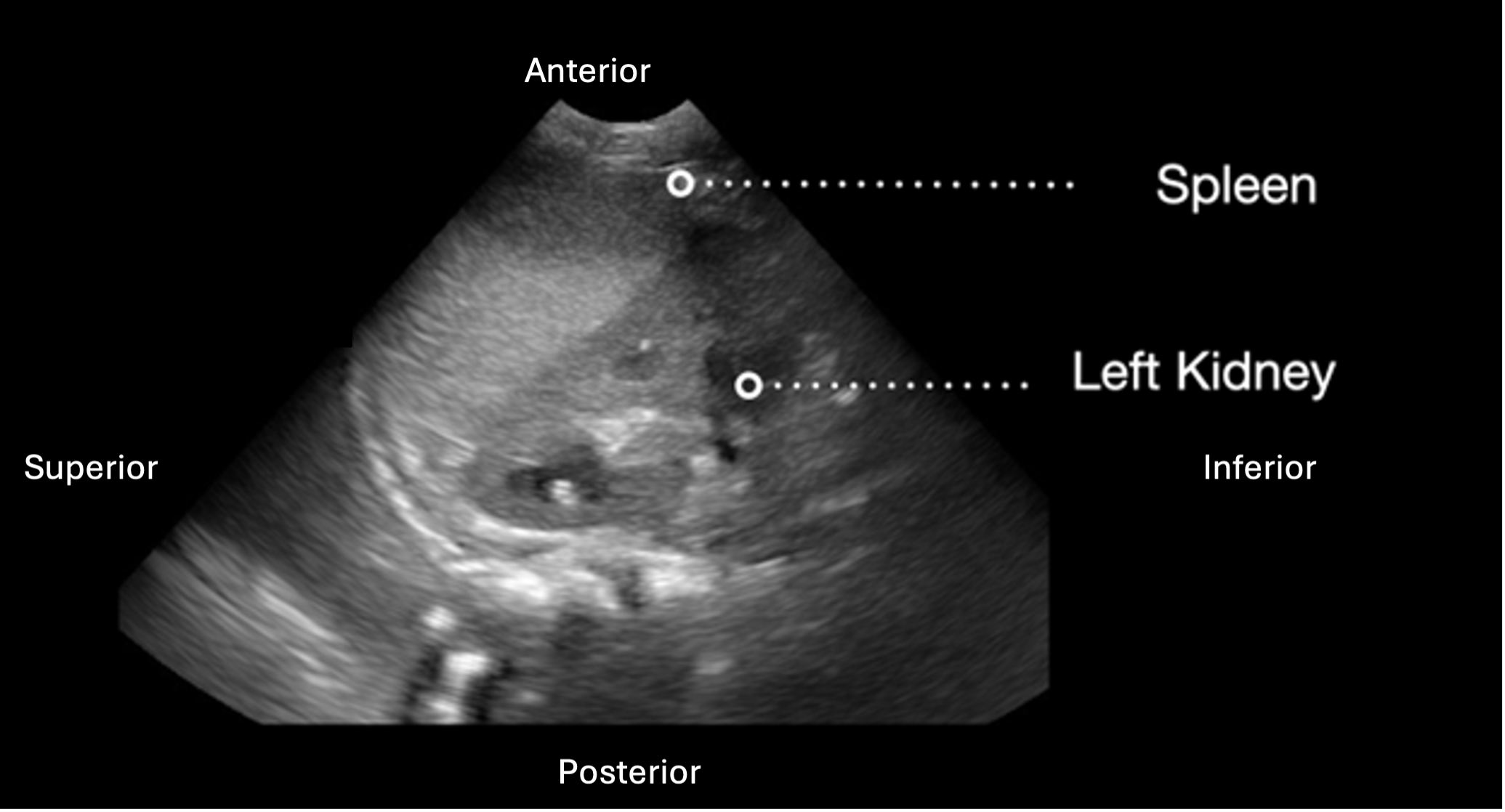 Figure 6: Longitudinal view of the left kidney with labeled image orientation and surrounding structures
Figure 6: Longitudinal view of the left kidney with labeled image orientation and surrounding structures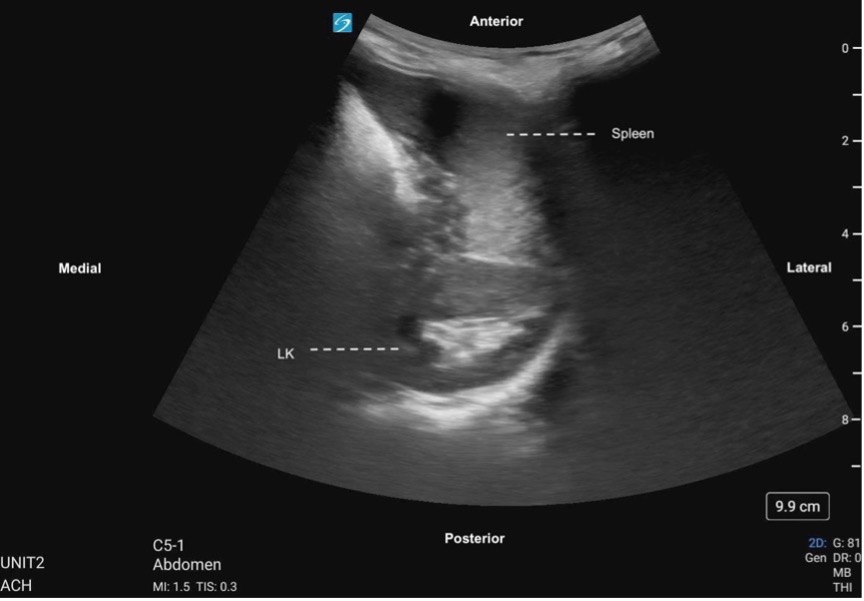 Figure 7. Left kidney transverse, labeled with image orientation and surrounding structures
Figure 7. Left kidney transverse, labeled with image orientation and surrounding structures

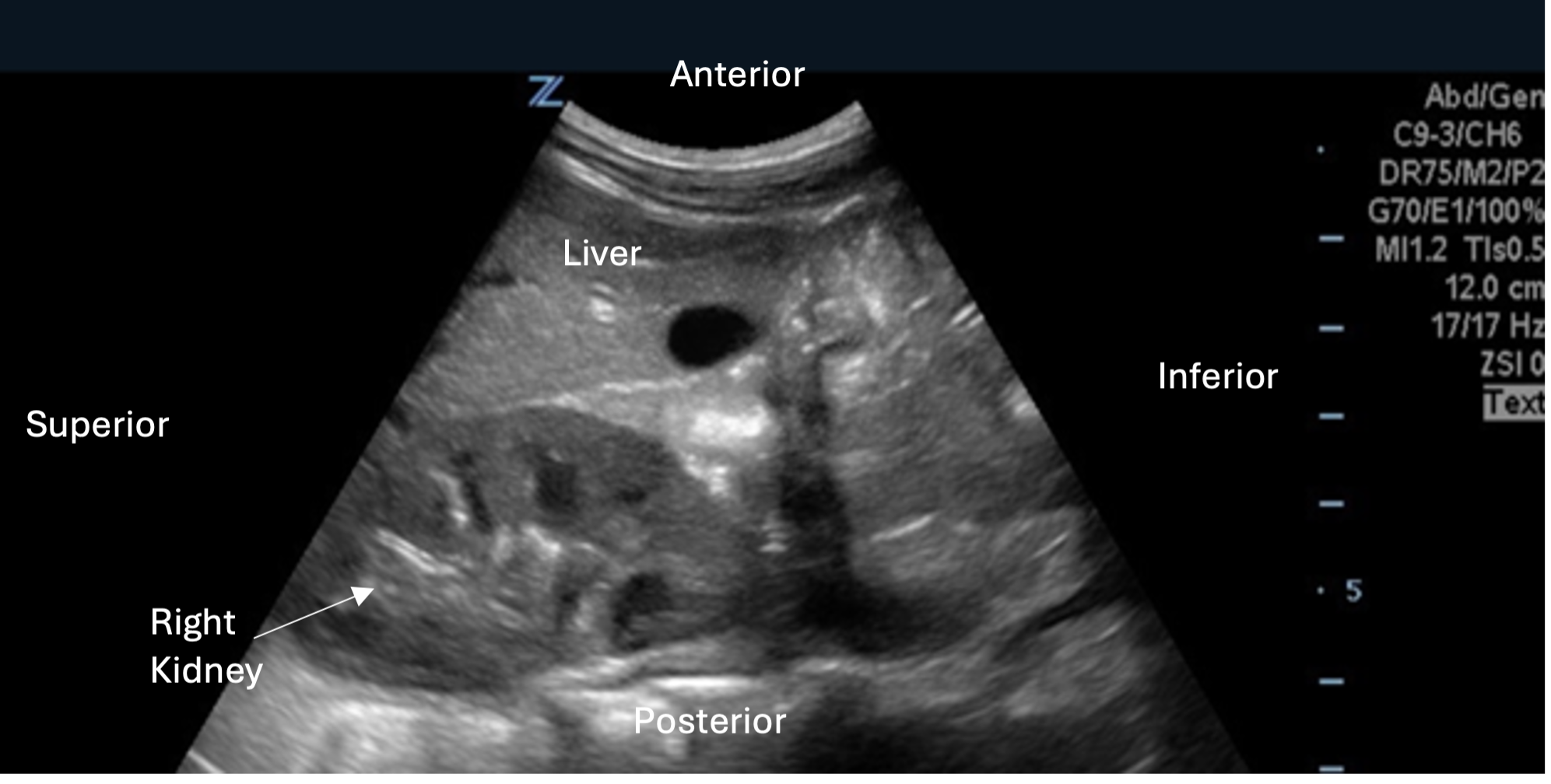 Figure 2. Longitudinal view of the right kidney with labeled image orientation and surrounding structures
Figure 2. Longitudinal view of the right kidney with labeled image orientation and surrounding structures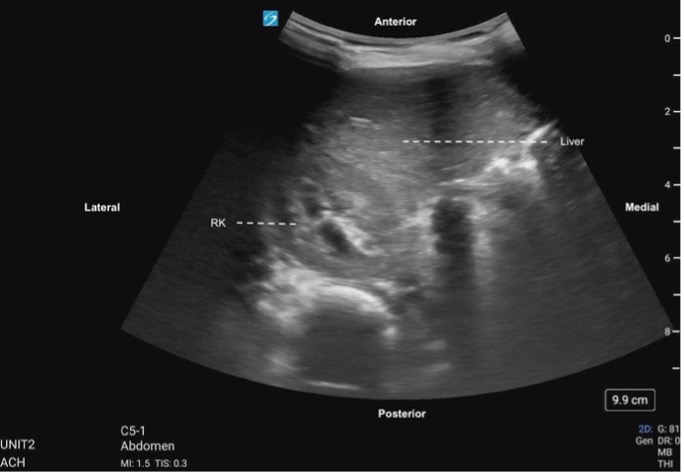 Figure 3. Right kidney transverse, labeled with image orientation and surrounding structures
Figure 3. Right kidney transverse, labeled with image orientation and surrounding structures