Technique
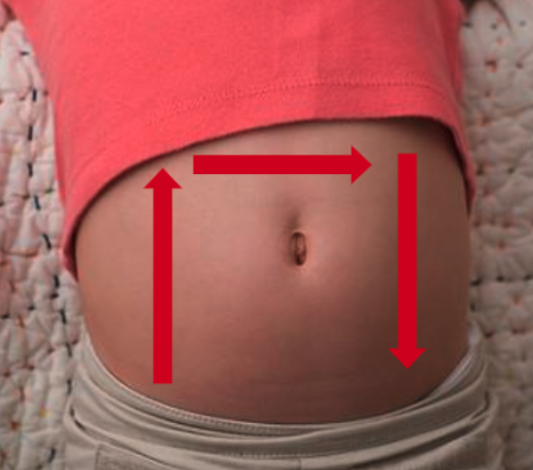
Figure 1: The inverted “U” technique to identify ileocolic intussusception
While several techniques have been described, we will focus on the one known as the “Inverted U” [figure 1]:
- With the patient supine and in a position of comfort (possibly in the parent’s lap) place probe in the right lower quadrant with the probe marker aimed to the patient’s right while in the transverse plane. The psoas muscle and iliac vessels can be identified as the starting landmark on the right of the screen.
- Move the probe laterally until the cecum is identified. From here you will follow the path of the large intestine to identify any evidence of intussusception.
- With the probe in the transverse plane, slowly move the probe superiorly to the right upper quadrant until the liver and gallbladder are visualized as landmarks—following the course of the large bowel.
- Rotate the probe 90 degrees clockwise so the probe marker is aimed toward the patient’s head and move the probe along the epigastrium to the left upper quadrant in the sagittal or longitudinal plane.
- Rotate the probe 90 degrees counterclockwise so the probe marker is pointed to the patient’s right and move the probe inferiorly towards the left lower quadrant.
- If an intussusception is visualized, confirm it’s presence in two planes, measure the AP diameter in the transverse plane and apply color Doppler to assess for blood flow and possible ischemia.
Scanning Tips:
– Graded compression can be applied to help displace bowel gas or air and improve visualization of intussusception.
– Intussusception is most often found just deep to the abdominal wall on the right side of the abdomen.