What am I Looking at?
In A4C view, you can assess LV wall motion at the basal, mid, and apical levels of the inferoseptal and anterolateral walls (figure 19). This view is also useful for visual estimation of overall contractility and evaluation of the LV’s size and shape throughout systole and diastole.
It is important to avoid foreshortening in the A4C view, as this can underestimate LV length and overestimate function. If the LV appears round or blunt at the apex, the image is likely foreshortened—slide the probe laterally and slightly inferiorly to better align with the cardiac apex, and angle it more anteriorly (toward the face) to bring the true apex into view and ensure a full-length chamber.
Formal echocardiography uses apical views to calculate EF using Simpson’s biplane methods; however, this is beyond the scope of PoCUS practice
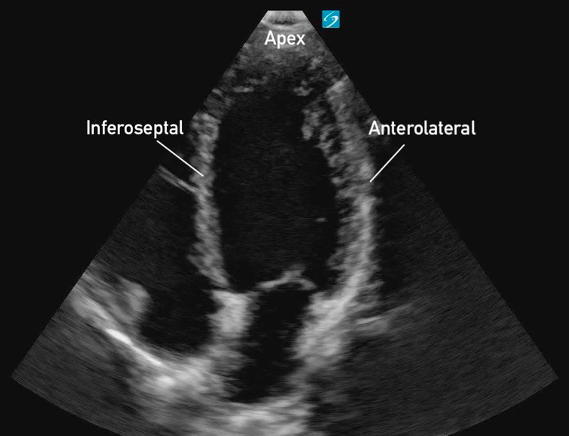 Figure 19: Apical 4 Chamber view in cardiology convention with the labeled left ventricular walls
Figure 19: Apical 4 Chamber view in cardiology convention with the labeled left ventricular walls
What is Normal
Contractility:
The apex and visible LV walls (inferoseptal and anterolateral) should move inward toward the center, with the base also moving toward the apex. All walls should demonstrate coordinated inward motion and uniform thickening.
Eyeballing Ejection Fraction:
When qualitatively assessing LV function in the A4C view, the EF can often be ‘eyeballed’. The LV cavity should visibly reduce its volume by more than half with each contraction. Longitudinal shortening will also contribute to overall cavity reduction.
Figure 20: A4C demonstrating adequate contractility despite poor window
Figure 21. A4C demonstrating adequate contractility and clear wall thickening
What is NOT Normal
Decreased global function:
LVfx is considered reduced if the visible walls fail to contract effectively toward the center of the cavity during systole. Wall motion appears sluggish or diminished, and the overall inward movement and thickening are reduced.
Figure 22. A4C view in a child with severe, globally reduced systolic function
RWMAs:
RWMAs may be observed in the inferoseptal wall, anterolateral wall, or apex, with segments showing hypokinesis, paradoxical motion, dyskinesis or akinesis while other segments contract normally (figure 23). The segments may also be reduced in a global fashion.
Figure 23: A4C view demonstrating moderately reduced LF systolic function and RWMAs of the inferoseptal and anterolateral walls.
Hyperdynamic function:
The inferoseptal and anterolateral walls may nearly or completely touch during systole, leading to near obliteration of the ventricular cavity (figure 24). This effect is often more pronounced at the apex, while the basal segments may not completely obliterate.
Figure 24. A4C view demonstrating hyperdynamic LV systolic function.