The right upper quadrant
The right upper quadrant view uses the liver as an acoustic window to identify free fluid within the abdominal cavity. This is one of the most important views of the abdominal FAST. Free fluid often accumulates in the RUQ as the right paracolic gutter directs fluid from the pelvis to the RUQ and the phrenicocolic ligament and mesentery direct fluid from the LUQ to RUQ.
Technique (figure 1)
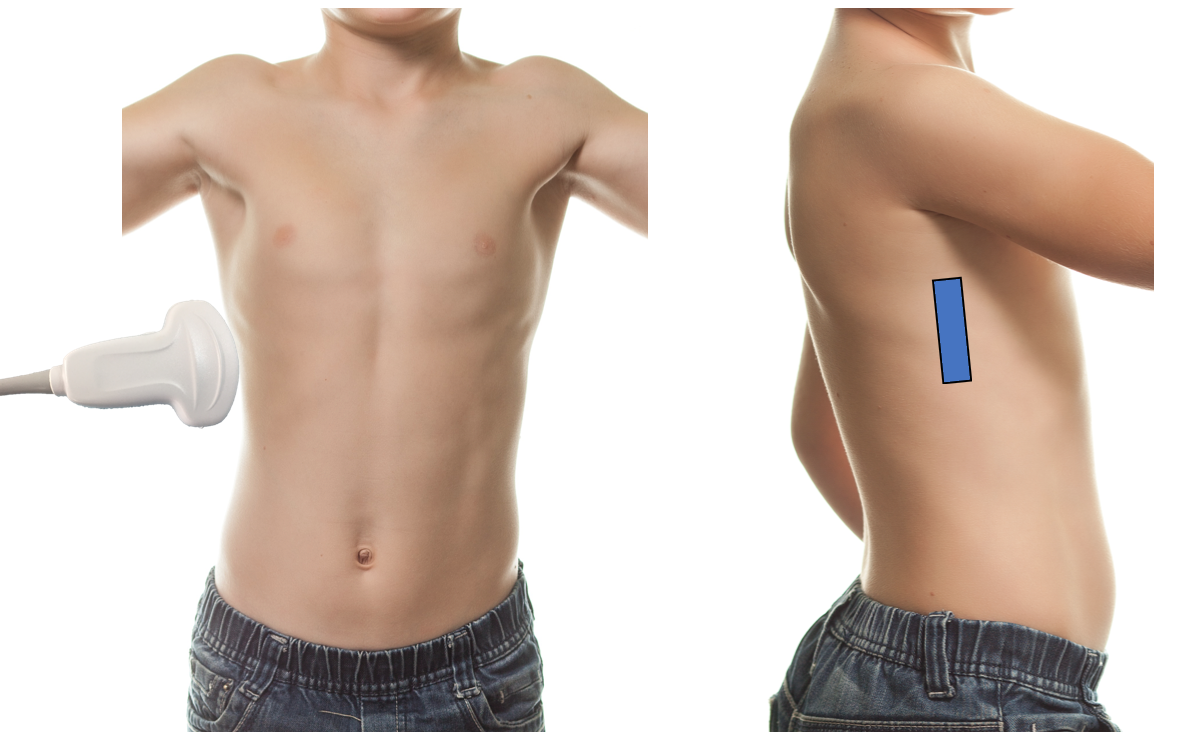
Figure 1: Scanning technique of the RUQ
- Positioning is critical. It is important that the patient remains supine in a flat or slight Trendelenburg position to ensure any fluid collects in dependent areas.
- Place the probe on the patient’s right mid-axillary line along the coronal plane at the level of the xyphoid with the probe indicator toward the patient’s head.
- Center the hepatorenal interface on the screen by moving up or down an intercostal space as needed.
- Draw your eye to the area below the diaphragm, hepatorenal interface and caudal liver tip to identify free fluid.
- Fan slowly from anterior to posterior and back until the kidney disappears in either direction, repeat in each view, as needed, to fully evaluate the subdiaphragmatic space, hepatorenal interface and caudal liver tip.
- Fluid will appear anechoic (black) on the screen.
Tips
- Fan through the area slowly so as not to miss subtle findings, drawing your eyes to the key areas of the hepatorenal interface and the caudal liver tip.
- It is common to have to fan in multiple rib spaces to ensure a view of the whole hepatorenal interface and caudal liver edge.
- If struggling to see between rib shadows, angle the probe slightly to follow the direction of the intercostal spaces to allow you to see between the ribs.
What am I looking at?
When placing the probe in the RUQ you are using the liver as an acoustic window to get a coronal cross section of the patient’s abdomen (figure 2).
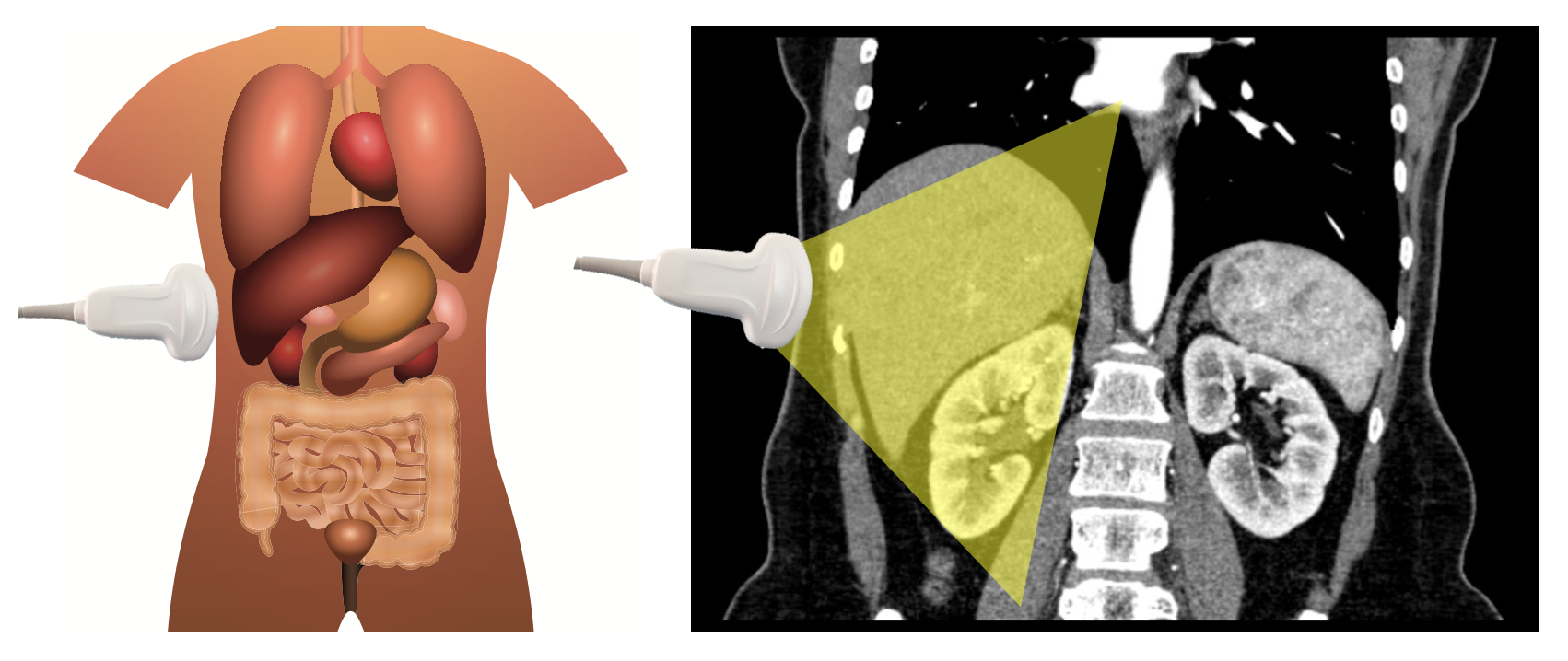
Figure 2: When scanning the right upper quadrant, use the liver as an acoustic window to get a coronal view of the liver, right kidney and hepatorenal interface.
What is normal?
Nearest to the probe, the lateral chest wall containing muscle and ribs is easily identified. Often, the hypoechoic rib shadows can be seen projecting into the abdomen. Deep to the chest wall the liver is encountered, followed by the hepatorenal interface and right kidney. The domed diaphragm can be seen cranial to the liver and the vertebral bodies and great vessels can often be identified in the far field deep to the kidney (figure 3, video 1).

Figure 3: Normal RUQ sonoanatomy with the liver highlighted in blue, right kidney in green, diaphragm in red and vertebral bodies in yellow. Your areas of interest include the sub-diaphragmatic space (1), Morrison’s pouch (2) and the liver tip (3).
Video 1: RUQ, normal
What is not normal?
When intraperitoneal free fluid is encountered due to infection, ascites or hemorrhage fluid often collects in right paracolic gutter around the caudal edge of the liver and in morrison’s pouch, or the hepatorenal interface (video 2 & 3). Fluid appears as an anechoic stripe or collection in these areas only bounded by the surrounding anatomical structures. In pediatric patients the second most common area for fluid to collect is in the right paracolic gutter adjacent to the caudal liver edge [11].
Video 2: RUQ, free fluid in Morrison’s pouch
Video 3: RUQ, free fluid around the caudal liver tip
Pitfalls
PoCUS for abdominal free fluid is not foolproof.
False negative scans are most commonly caused by operator error. Other causes include patients who only have small amounts of fluid in their abdomen, such as trauma patients presenting early or with minimal hemorrhage. In addition, in trauma patients with delayed presentations, blood can clot which can prevent it from collecting in dependent regions or can make it harder to distinguish on ultrasound (due to the variable echogenicity of clotted blood).
False positives can occur as well, most commonly due to perinephric fat or edge artifact. In the case of perinephric fat, free fluid can often be distinguished as anechoic as opposed to hypoechoic, as fat is. In addition, free fluid is bound only by the organs themselves, while perinephric fat is lined by apparent hyperechoic fascial lines giving a “railroad track” or “marbled” appearance. Edge artifact can sometimes be seen projecting from the edge of a curved structure, usually the kidney; it often is less distinct than free fluid, gets larger as it goes deeper and crosses anatomical boundaries—similar to a rib shadow, whereas free fluid tends to be anechoic, well-defined and narrows to dissect planes and respects anatomic boundaries.