Parasternal Short Axis (PSAX/PSSA)
The PSAX view provides a cross-sectional image of the ventricles, allowing simultaneous visualization of the RV and LV. For RV strain assessment, this view is useful for evaluating RV size, function. It is also the preferred view to assess the shape and position of the IVS.
The RV appears as a crescent-shaped structure anteriorly, wrapping around the circular LV cavity, with the septum forming a smooth, curved border between the two chambers (figure 8).
What is Normal?
- Crescent shaped
- Smaller than the LV
- In a normal PSAX view, the septum maintains a round, inward curvature toward the RV throughout the cardiac cycle.
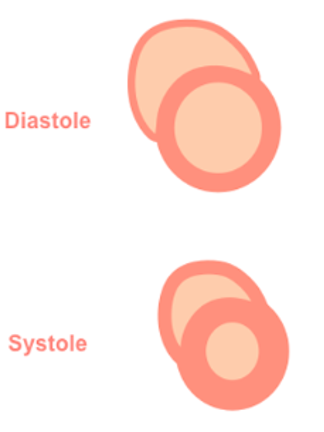
Figure 7: Illustration of normal septal shape during systole and diastole in the PSAX view
Figure 8: PSAX view. Note how the septum maintains its round inward curvature during throughout the entire cardiac cycle and the crescent shape of the RV in the near field.
What is NOT Normal?
- Visually, if the RV is equal to or larger than the LV, then there is likely RV dilation. In severely dilated RVs, the LV will appear to look compressed by the RV
- Visually reduced contraction
- Septal flattening or becoming D-shaped when RV pressure > LV pressure
Septal Flattening
In the PSAX view, the LV will appear as a “D-shaped” structure. This is the result of RV volume overload (RVVO) or RV pressure overload (RVPO).
· In RVVO the septum is flattened only during diastole. This is the result of elevated RV volume filling at the expense of the LV, and causes the LV shape to deform by the end of diastole
· In RVPO the septum will be flattened throughout the entire cardiac cycle.
It is important to remember that to accurately assess septal position, the PSAX view should be obtained at the level of the papillary muscles, rather than at the mitral valve. At the mitral valve level, surrounding structures may artificially preserve septal shape despite significant RV loading.
It is also important to note that intra-cardiac shunts (e.g., VSDs) and arrhythmias can also limit the reliability of RV/LV and septal assessments in the PSAX view.
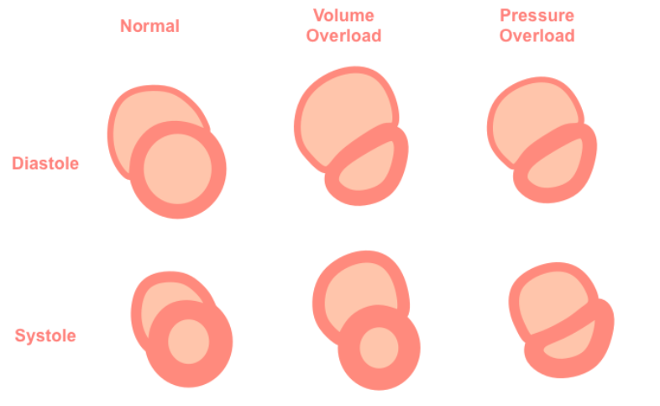
Figure 9: Illustration of Septal flattening or “D-sign” as seen in the PSAX view
Figure 10: PSAX view “D-sign” throughout cardiac cycle indicative of RVVO/RVPO